


The thyroid gland, located in the anterior neck just below the cricoid cartilage, consists of 2 lobes connected by an isthmus. Follicular cells in the gland produce the 2 main thyroid hormones:
Tetraiodothyronine (thyroxine, T4)
Triiodothyronine (T3)
These hormones act on cells in virtually every body tissue by combining with nuclear receptors and altering expression of a wide range of gene products. Thyroid hormone is required for normal brain and somatic tissue development in the fetus and neonate, and, in people of all ages, thyroid hormone regulates protein, carbohydrate, and fat metabolism.
T4 has minimal hormonal activity, but its long half-life (8 days) serves as a reservoir or prohormone for T3. T4 is converted (in most tissues) to T3, the active form that binds to nuclear receptors, and to reverse T3 (rT3), an inactive form of thyroid hormone without metabolic activity. Levels of rT3 increase in certain diseases.
Parafollicular cells (C cells) in the thyroid secrete the hormone calcitonin, which is released in response to hypercalcemia and lowers serum calcium levels (see Regulation of Calcium Metabolism).
Synthesis and Release of Thyroid Hormones
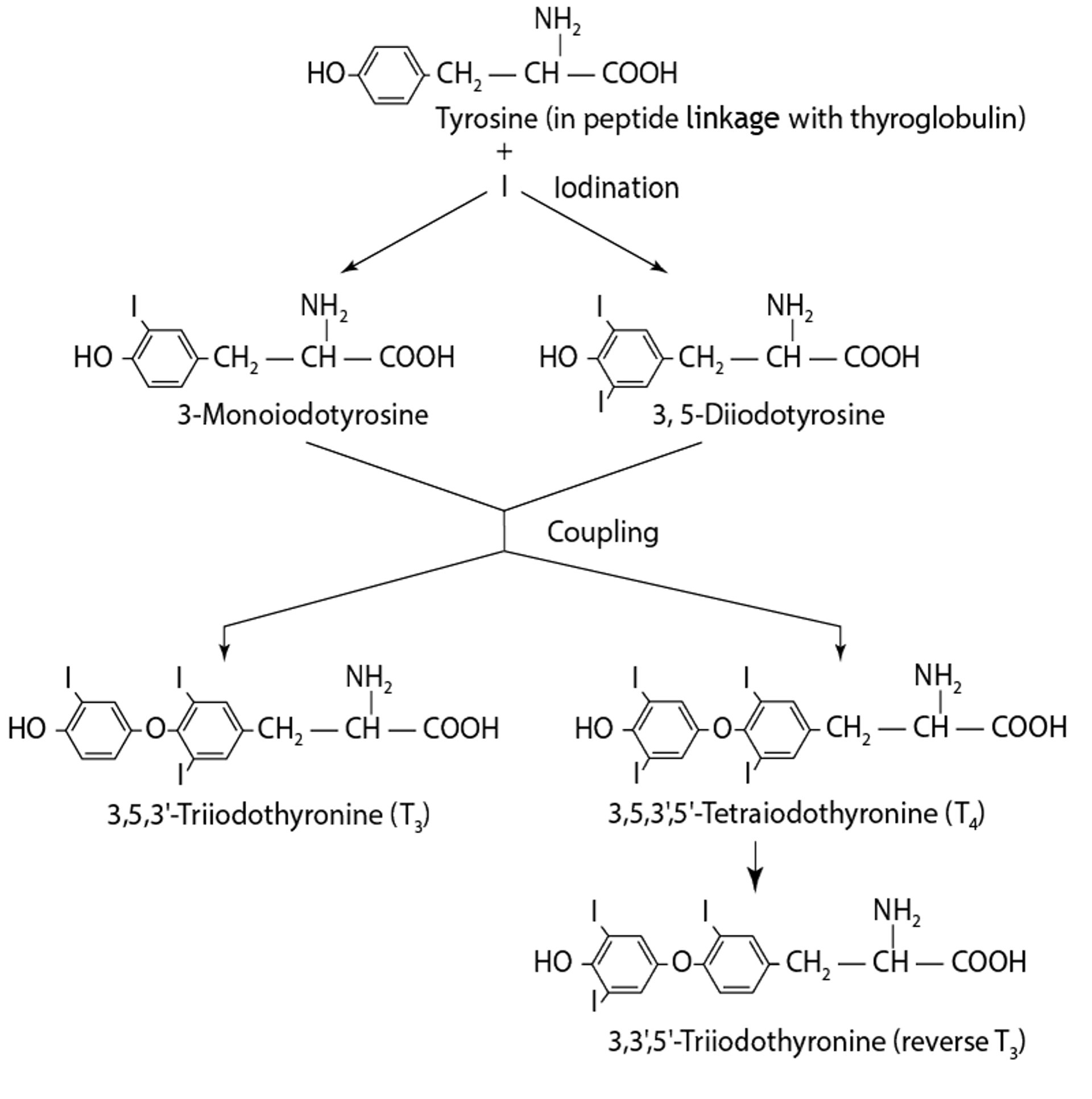
Synthesis of thyroid hormones requires iodine (see figure Synthesis of Thyroid Hormones). Iodine, ingested in food and water as iodide, is actively concentrated by the thyroid and converted to organic iodine (organification) within follicular cells by thyroid peroxidase. The follicular cells surround a space (follicle) filled with colloid, which consists of thyroglobulin, a glycoprotein containing tyrosine within its matrix. Tyrosine in contact with the membrane of the follicular cells is iodinated at 1 (monoiodotyrosine) or 2 (diiodotyrosine) sites and then coupled to produce the 2 forms of thyroid hormone.
Diiodotyrosine + diiodotyrosine → T4
Diiodotyrosine + monoiodotyrosine → T3
Synthesis of Thyroid Hormones

T3 and T4 remain incorporated in thyroglobulin within the follicle until the follicular cells take up thyroglobulin as colloid droplets. Once inside the thyroid follicular cells, T3 and T4 are cleaved from thyroglobulin.
Free T3 and T4 are then released into the bloodstream, where they are bound to serum proteins for transport. The primary transport protein is thyroxine-binding globulin (TBG), which has high affinity but low capacity for T3 and T4. TBG normally carries approximately 75% of bound thyroid hormones.
The other binding proteins are
Thyroxine-binding prealbumin (transthyretin), which has high affinity but low capacity for T4
Albumin, which has low affinity but high capacity for T3 and T4
Approximately 0.3% of total serum T3 and 0.03% of total serum T4 are free and in equilibrium with bound hormones. Only free T3 and free T4 are available to act on the peripheral tissues.
All reactions necessary for the formation and release of T3 and T4 are controlled by thyroid-stimulating hormone (TSH), which is secreted by pituitary thyrotropic cells. TSH secretion is controlled by a negative feedback mechanism in the pituitary: Increased levels of free T4 and T3 inhibit TSH synthesis and secretion, whereas decreased levels increase TSH secretion. TSH secretion is also influenced by thyrotropin-releasing hormone (TRH), which is synthesized in the hypothalamus. The precise mechanisms regulating TRH synthesis and release are unclear, although negative feedback from thyroid hormones inhibits TRH synthesis.
Most circulating T3 is produced outside the thyroid in peripheral tissues by monodeiodination of T4. Only one fifth of circulating T3 is secreted directly by the thyroid.
Laboratory Testing of Thyroid Function
Thyroid-stimulating hormone (TSH) measurement
TSH measurement is the best means of determining thyroid dysfunction (see table Results of Thyroid Function Tests in Various Clinical Situations). Normal TSH levels rule out hyperthyroidism or hypothyroidismEuthyroid Sick Syndrome) .
Changes in the serum TSH level in the presence of normal levels of serum T4, free T4, serum T3, and free T3 define the syndromes of subclinical hyperthyroidism (low serum TSH) and subclinical hypothyroidism (elevated serum TSH).
Thyroxine (T4) measurement
Total serum T4 is a measure of bound and free hormone. Changes in levels of thyroid hormone–binding serum proteins (TBG or albumin) produce corresponding changes in total T4, even though levels of physiologically active free T4 are unchanged. Thus, a patient may have physiologically normal free T4 levels but have an abnormal total serum T4 level. Free T4 in the serum can be measured directly, avoiding the pitfalls of interpreting total T4 levels.
Free T4 index is a calculated value that corrects total T4 for the effects of varying amounts of thyroid hormone–binding serum proteins and thus gives an estimate of free T4 when total T4 is measured. The thyroid hormone–binding ratio or T4 resin uptake is used to estimate protein binding. Free T4 index is readily available and compares well with direct measurement of free T4.
Triiodothyronine (T3) measurement
Total serum T3 and free T3 can also be measured. Because T3 is tightly bound to TBG (although 10 times less so than T4), total serum T3 levels are influenced by alterations in serum TBG level and by medications that affect binding to TBG. Free T3 levels in the serum are measured by the same direct and indirect methods (free T3 index) described for T4 and are used mainly for evaluating thyrotoxicosis.
Thyroxine-binding globulin (TBG)
TBG can be measured. It is increased in pregnancy, by estrogen therapy, or by use of estrogen-progestin oral contraceptives, and in the acute phase of infectious hepatitis. TBG may also be increased by an X-linked mutation in the gene encoding TBG. It is most commonly decreased by illnesses that reduce hepatic protein synthesis, use of anabolic steroids, the nephrotic syndrome, and excessive corticosteroid use. Large doses of certain medications, such as phenytoin and aspirin and their derivatives, displace T4 from its binding sites on TBG, which spuriously lowers total serum T4 levels.
Autoantibodies to thyroid peroxidase
Autoantibodies to thyroid peroxidase are present in almost all patients with Hashimoto thyroiditis (some of whom also have autoantibodies to thyroglobulin) and in most patients with Graves disease. These autoantibodies are markers of autoimmune disease but probably do not cause disease. However, an autoantibody directed against the thyroid-stimulating hormone receptor (thyroid-stimulating immunoglobulin [TSI]) on the thyroid follicular cell is responsible for the hyperthyroidism in Graves disease. Antibodies against T4 and T3 may be found in patients with autoimmune thyroid disease and may affect T4 and T3 measurements but are rarely clinically significant.
Thyroglobulin
The thyroid is the only source of thyroglobulin, which is readily detectable in the serum of healthy people and is usually elevated in patients with nontoxic or toxic (producing thyroid hormone and causing symptomatic hyperthyroidism) goiter. The principal use of serum thyroglobulin measurement is in evaluating patients after near-total or total thyroidectomy (with or without iodine-131 ablation) for differentiated thyroid cancer. Normal or elevated serum thyroglobulin values indicate the presence of residual normal or cancerous thyroid tissue in patients receiving TSH-suppressive doses of levothyroxine or after withdrawal of levothyroxine. However, thyroglobulin antibodies interfere with thyroglobulin measurement.
Screening for Thyroid Dysfunction
Screening for thyroid disease is recommended in many states and countries for all newborns to detect congenital hypothyroidism, which may impair normal development if untreated (1).
Routine screening for asymptomatic adults, including pregnant women without known risk factors for thyroid disease, is not recommended due to insufficient evidence of a benefit (2). For patients with risk factors, the serum TSH should be measured and is the best test to screen for both hyperthyroidism and hypothyroidism.
Because of the increased prevalence of subclinical hypothyroidism (defined as elevated serum TSH but normal T4 levels) in older adults, some authorities recommend screening on an annual basis for those > age 70 years, although serum TSH level has been shown to increase with age without indicating disease. This increase has led to overtreatment in up to 40% of patients (3), so it is uncertain whether treating older adults in whom subclinical hypothyroidism has been detected has any benefit.
Screening references
1. Rose SR, Wassner AJ, Wintergerst KA, et al. Congenital Hypothyroidism: Screening and Management. Pediatrics 2023;151(1):e2022060420. doi:10.1542/peds.2022-060420
2. Thyroid Disease in Pregnancy: ACOG Practice Bulletin, Number 223. Obstet Gynecol 2020;135(6):e261-e274. doi:10.1097/AOG.0000000000003893
3. Somwaru LL, Arnold AM, Joshi N, Fried LP, Cappola AR. High frequency of and factors associated with thyroid hormone over-replacement and under-replacement in men and women aged 65 and over. J Clin Endocrinol Metab 2009;94(4):1342-1345. doi:10.1210/jc.2008-1696
Radioactive Iodine Uptake and Imaging
Radioactive iodine uptake can be measured. A trace amount of radioiodine is given orally or intravenously; a scanner then detects the amount of radioiodine taken up by the thyroid. The preferred radioiodine isotope is iodine-123, which exposes the patient to minimal radiation (much less than iodine-131). Thyroid iodine-123 uptake varies widely with iodine ingestion and is low in patients exposed to excess iodine.
The test is valuable in the differential diagnosis of hyperthyroidism (high uptake in Graves disease, low uptake in thyroiditis). It may also help in the calculation of the dose of iodine-131 needed for treatment of hyperthyroidism.
Imaging using a scintillation camera can be done after radioisotope administration (radioiodine or technetium 99m pertechnetate) to produce a graphic representation of isotope uptake. Focal areas of increased (hot) or decreased (cold) uptake help distinguish areas of possible cancer (thyroid cancers exist in < 1% of hot nodules compared with 10 to 20% of cold nodules).






