


In adrenal insufficiency, the adrenal glands do not produce enough adrenal hormones.
Adrenal insufficiency may be caused by a disorder of the adrenal glands, a disorder of the pituitary gland, or by certain medications.
Adrenal insufficiency may be caused by an autoimmune reaction, cancer, an infection, or some other disease.
A person with adrenal insufficiency feels weak, tired, and dizzy when standing up after sitting or lying down, and may develop dark skin patches.
Doctors measure sodium and potassium in the blood and measure cortisol and adrenocorticotropic hormone (ACTH) levels to make the diagnosis.
People are given corticosteroids and fluids.
(See also Overview of the Adrenal Glands.)
Adrenal insufficiency may be:
Primary (Addison disease, a disorder of the adrenal glands themselves)
Secondary (a disorder affecting the pituitary gland, which controls the adrenal glands)
In both types of adrenal insufficiency, the adrenal glands produce an inadequate amount of one or more adrenal hormones.
Adrenal hormones
When the adrenal glands become underactive, they tend to produce inadequate amounts of all of the adrenal hormones, including corticosteroids (particularly cortisol) and mineralocorticoids (particularly aldosterone, which controls blood pressure and the levels of salt [sodium chloride] and potassium in the body). The adrenal glands also produce small amounts of testosterone and estrogen and other similar sex hormones (androgens, such as dehydroepiandrosterone [DHEA]), levels of which also are reduced in people with adrenal insufficiency.
Thus, insufficient adrenal hormones can affect the balance of water, sodium, and potassium in the body, as well as the body’s ability to control blood pressure and react to stress. In addition, loss of androgens may cause a loss of body hair in women. In men, testosterone from the testes more than makes up for this loss. DHEA may have additional effects that do not relate to androgens.
When the adrenal glands are destroyed by infection or cancer, the adrenal medulla and thus the source of epinephrine, is also lost. However, this loss does not cause symptoms.
A deficiency of aldosterone, in particular, causes the body to excrete large amounts of sodium and retain potassium, leading to low levels of sodium and high levels of potassium in the blood. The kidneys are not able to retain sodium easily, so a person loses too much sodium, the level of sodium in the blood falls, and the person becomes dehydrated. Severe dehydration and a low sodium level reduce blood volume and can lead to shock.
Corticosteroid deficiency leads to an extreme sensitivity to insulin so that the level of sugar in the blood may fall dangerously low (hypoglycemia). The deficiency prevents the body from manufacturing carbohydrates, which are needed for cells to function, and protein, for fighting infections properly and controlling inflammation. Muscles weaken, and even the heart can become weak and unable to pump blood adequately. In addition, the blood pressure may become dangerously low.
People with adrenal insufficiency are not able to produce the additional corticosteroids that are needed when the body is stressed. People therefore are susceptible to serious symptoms and complications when confronted with illness, extreme fatigue, severe injury, surgery, or, possibly, severe psychologic stress.
Primary adrenal insufficiency (Addison disease)
Addison disease can start at any age and affects men and women about equally.
In 70% of people with Addison disease, the cause is not precisely known, but the adrenal glands are affected by an autoimmune reaction in which the body’s immune system attacks and destroys the adrenal cortex (the outer part of the gland, which is distinct from the adrenal medulla, the inner part which produces different hormones).
In the other 30%, the adrenal glands are destroyed by cancer, an infection such as tuberculosis, or another identifiable disease. In infants and children, Addison disease may be due to a genetic abnormality of the adrenal glands (see Congenital adrenal hyperplasia).
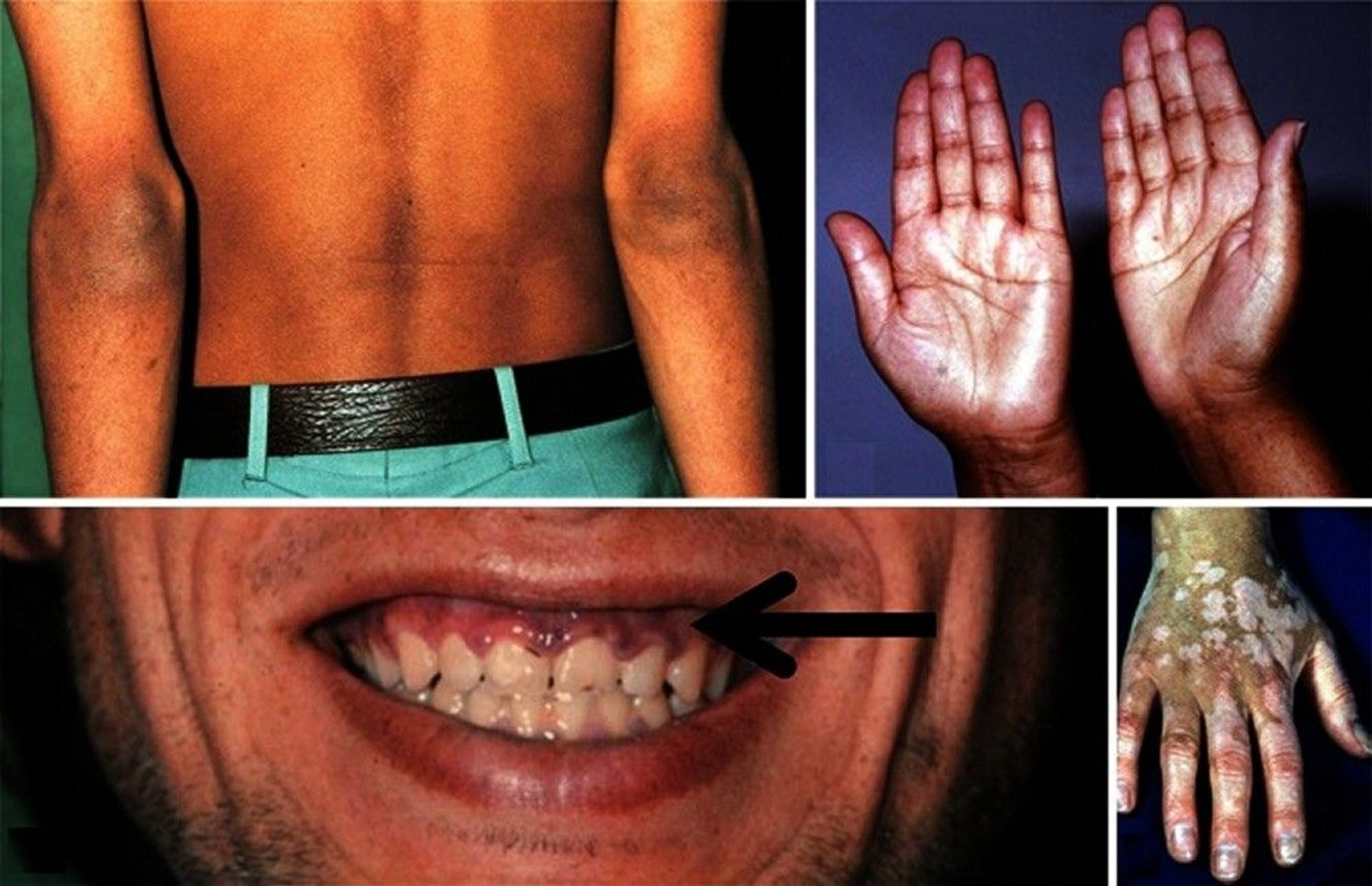
In Addison disease, the pituitary gland produces more adrenocorticotropic hormone (ACTH, also known as corticotropin) in an attempt to stimulate the adrenal glands. ACTH also stimulates melanin production, so the skin and the lining of the mouth often develop a dark pigmentation.
Secondary adrenal insufficiency
Secondary adrenal insufficiency is a term given to a disorder that resembles Addison disease. In this disorder, the adrenal glands are underactive because the pituitary gland produces less ACTH, not because the adrenal glands have been destroyed or have otherwise directly failed. Lack of ACTH affects adrenal secretion of cortisol much more than secretion of aldosterone.
The pituitary gland may fail to produce ACTH because of a tumor, an infection, or an injury. Also, taking corticosteroid medications for more than a few weeks keeps the pituitary gland from producing enough ACTH, so the adrenal glands are not stimulated adequately.
Symptoms of secondary adrenal insufficiency are similar to those of Addison disease except that patches of darker skin are absent, and dehydration does not usually occur. Secondary adrenal insufficiency is diagnosed by blood tests. Unlike in Addison disease, sodium and potassium levels tend to be near normal in secondary adrenal insufficiency, and the ACTH level is low.
Symptoms of Adrenal Insufficiency
People with adrenal insufficiency feel weak, tired, and dizzy when standing up after sitting or lying down. These problems may develop gradually and insidiously.
People with Addison disease develop patches of dark skin. The darkness may seem like tanning, but it appears on areas that are not exposed to the sun. People with dark skin can also develop excessive pigmentation, although the change may be harder to recognize. Dark freckles may develop over the forehead, face, and shoulders, and a bluish black discoloration may develop around the nipples, lips, mouth, rectum, scrotum, or vagina. Dark skin patches usually do not occur in people with secondary adrenal insufficiency.

© Springer Science+Business Media
Most people lose weight, become dehydrated, have no appetite, and develop muscle aches, nausea, vomiting, and diarrhea. Many become unable to tolerate cold. Unless the disease is severe, symptoms tend to become apparent only during times of stress. Periods of hypoglycemia, with nervousness and extreme hunger for salty foods, can occur, particularly in children.
Adrenal crisis
If adrenal insufficiency is not treated, an adrenal crisis may occur. Severe abdominal pain, profound weakness, extremely low blood pressure, kidney failure, and shock may occur. An adrenal crisis often occurs if the body is subjected to stress, such as an accident, injury, surgery, or severe infection. If adrenal crisis is not treated, it may be fatal.
Diagnosis of Adrenal Insufficiency
Blood tests
Because the symptoms may start slowly and subtly, and because no single laboratory test may give definitive results in the early stages, doctors often do not suspect adrenal insufficiency at the outset. Sometimes a major stress makes the symptoms more obvious and precipitates a crisis.
Blood tests may show low sodium and high potassium levels and usually indicate that the kidneys are not working well. Doctors who suspect adrenal insufficiency measure cortisol levels, which may be low, and ACTH levels. ACTH levels tend to be high in primary adrenal insufficiency and low in secondary adrenal insufficiency. However, doctors may need to confirm the diagnosis by measuring cortisol levels before and after an injection of a synthetic form of ACTH. If cortisol levels are low, further tests are needed to determine if the problem is Addison disease or secondary adrenal insufficiency.
Treatment of Adrenal Insufficiency
Corticosteroids
cortisolhydrocortisone intravenously or intramuscularly at first and then hydrocortisone tablets. Because the body normally produces most cortisol in the morning, replacement hydrocortisone should also be taken in divided doses, with the largest dose in the morning. Hydrocortisone will need to be taken every day for the rest of the person’s life. Larger doses of hydrocortisone are needed when the body is stressed, especially as a result of an illness, and may need to be given by injection if the person has severe diarrhea or vomiting.
testosterone is not usually needed, although there is some evidence that replacement with DHEA improves the quality of life in some people. Although treatment must be continued for life, the outlook is excellent.






