


Dyslipidemia is a high level of cholesterol and/or triglycerides or a low level of high-density lipoprotein (HDL) cholesterol.
Lifestyle, genetics, disorders (such as low thyroid hormone levels or kidney disease), medications, or a combination can contribute.
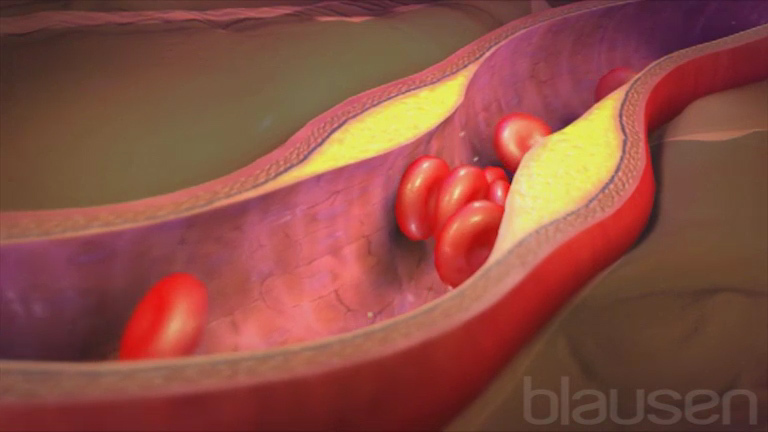
Atherosclerosis can result, causing angina, heart attacks, strokes, and peripheral arterial disease.
Doctors measure levels of triglycerides and the various types of cholesterol in the blood.
Exercise, dietary changes, and drugs can be effective.
(See also Overview of Cholesterol and Lipid Disorders.)
Important fats (lipids) in the blood are
Cholesterol
Triglycerides
Cholesterol is an essential component of cell membranes, of brain and nerve cells, and of bile, which helps the body absorb fats and fat-soluble vitamins. The body uses cholesterol to make vitamin D and various hormones, such as estrogen, testosterone, and cortisol. The body can produce all the cholesterol that it needs, but it also obtains cholesterol from food.
Triglycerides, which are contained in fat cells, can be broken down, then used to provide energy for the body’s metabolic processes, including growth. Triglycerides are produced in the intestine and liver from smaller fats called fatty acids. Some types of fatty acids are made by the body, but others must be obtained from food.
Lipoproteins are particles of proteins and other substances. They carry fats, such as cholesterol and triglycerides, which cannot circulate freely in the blood by themselves.
There are different types of lipoproteins (see table Lipoproteins: Lipid Carriers), including
Chylomicrons
High-density lipoproteins (HDL)
Low-density lipoproteins (LDL)
Very low density lipoproteins (VLDL)
Levels of lipoproteins and therefore lipids, particularly low-density lipoprotein (LDL) cholesterol, increase slightly as people age. Levels are normally slightly higher in men than in women, but levels increase in women after menopause. The increase in levels of lipoproteins that occurs with age can result in dyslipidemia.
The risk of developing atherosclerosis increases as the total cholesterol level (which includes LDL cholesterol, HDL cholesterol, and VLDL cholesterol) increases, even if the level is not high enough to be considered dyslipidemia. Atherosclerosis can affect the arteries that supply blood to the heart (causing coronary artery disease), those that supply blood to the brain (causing stroke), and those that supply the rest of the body (causing peripheral arterial disease). Therefore, having a high total cholesterol level also increases the risk of having a heart attack or stroke.
Having a low total cholesterol level is generally considered better than having a high one. However, having a very low cholesterol level may not be healthy either (hypolipidemia).
Although there is no natural cutoff between normal and abnormal cholesterol levels, for adults, a total cholesterol level of less than 200 milligrams per deciliter of blood (mg/dL [< 5.1 mmol/L]) is desirable. And many people benefit from keeping the lipid level even lower. In parts of the world (such as China and Japan) where the average cholesterol level is 150 mg/dL (3.8 mmol/L), coronary artery disease is less common than it is in countries such as the United States. The risk of a heart attack more than doubles when the total cholesterol level approaches 300 mg/dL (7.7 mmol/L).
The total cholesterol level is only a general guide to the risk of atherosclerosis. Levels of the components of total cholesterol—particularly LDL and HDL cholesterol—are more important. A high level of LDL (bad) cholesterol increases the risk. A high level of HDL (good) cholesterol is not usually considered a disorder because it decreases the risk of atherosclerosis. However, a low level of HDL cholesterol (defined as less than 40 mg/dL [less than 1 mmol/L]) is associated with increased risk. Experts consider an LDL cholesterol level of less than 100 mg/dL (2.6 mmol/L) desirable.
Whether high triglyceride levels increase the risk of a heart attack or stroke is uncertain. Triglyceride levels higher than 150 mg/dL (1.7 mmol/L) are considered abnormal, but high levels do not appear to increase risk for everyone. For people with high triglyceride levels, the risk of heart attack or stroke is increased if they also have a low HDL cholesterol level, diabetes, chronic kidney disease, or many close relatives who have had atherosclerosis (family history).
A high level of HDL—the good—cholesterol may be beneficial and is not considered a disorder. A level that is too low increases the risk of atherosclerosis.
Lipoprotein (a) is a combination of LDL with an additional protein attached to it. Levels higher than about 30 mg/dL (or 75 nmol/L) are associated with increased risk of atherosclerosis. High levels are inherited. Lipoprotein (a) is not affected by diet or most lipid-lowering drugs. It usually only needs to be measured once.
Causes of Dyslipidemia
Factors that cause dyslipidemia are categorized into
Primary causes: Genetic (hereditary) causes
Secondary causes: Lifestyle and other causes
Both primary and secondary causes contribute to dyslipidemia in varying degrees. For example, a person with a hereditary hyperlipidemia may have even higher lipid levels if the person also has secondary causes of hyperlipidemia.
Primary (hereditary) dyslipidemia
Primary causes involve gene mutations that cause the body to produce too much LDL cholesterol or triglycerides or to fail to remove those substances. Some causes involve underproduction or excessive removal of HDL cholesterol. Primary causes tend to be inherited and thus to run in families. Some of the genetic causes of dyslipidemia are discussed here and elsewhere in THE MANUAL.
Cholesterol and triglyceride levels are highest in people with primary dyslipidemias, which interfere with the body’s metabolism and elimination of lipids. People can also inherit a tendency for HDL cholesterol to be unusually low.
Consequences of primary dyslipidemias can include premature atherosclerosis (in men 55 years old or younger, in women 60 years old or younger), which can lead to angina or heart attacks. Peripheral arterial disease is also a consequence, often causing decreased blood flow to the legs, with pain during walking (claudication). Stroke is another possible consequence. Very high triglyceride levels can cause pancreatitis.
In people who have a genetic disorder that causes high triglyceride levels (such as familial hypertriglyceridemia or familial combined hyperlipidemia), certain disorders and substances can increase triglycerides to extremely high levels. Examples of disorders include poorly controlled diabetes and chronic kidney disease. Examples of substances include excessive alcohol consumption and use of certain medications, such as estrogens (taken by mouth), that increase triglyceride levels.
Symptoms can include fatty deposits (eruptive xanthomas) in the skin on the front of the legs and back of the arms, enlargement of the spleen and liver, abdominal pain, and decreased sensitivity to touch due to nerve damage. Primary dyslipidemias can cause pancreatitis, which is occasionally fatal.
Limiting fat intake (to less than 50 grams a day) can help prevent nerve damage and pancreatitis. Losing weight and not drinking alcohol can also help. Lipid-lowering drugs may be effective.
Familial combined hyperlipidemia
In familial combined hyperlipidemia, the levels of cholesterol, triglycerides, or both may be high. This disorder affects about 1 to 2% of people. The lipid levels typically become abnormal after age 30 but sometimes at a younger age, especially in people who are overweight, who have a diet that is very high in fat, or who have metabolic syndrome.
Treatment of familial combined hyperlipidemia involves limiting intake of saturated fat, cholesterol, and sugar as well as exercising and, when applicable, losing weight. Many people with this disorder need to take lipid-lowering drugs.
Familial dysbetalipoproteinemia
In familial dysbetalipoproteinemia, levels of very low density lipoprotein (VLDL) cholesterol, total cholesterol, and triglycerides are high. These levels are high because an unusual form of VLDL accumulates in the blood. Fatty deposits (eruptive xanthomas) may form in the skin over the elbows and knees and in the palms, where they can cause yellow creases. This uncommon disorder results in the early development of severe atherosclerosis. By middle age, atherosclerosis often produces blockages in the coronary and peripheral arteries.
Treatment of familial dysbetalipoproteinemia involves achieving and maintaining recommended body weight and limiting intake of cholesterol, saturated fats, and carbohydrates. A lipid-lowering drug is usually needed. With treatment, lipid levels can be improved, the progression of atherosclerosis may be slowed, and the fatty deposits in the skin may become smaller or disappear.
Familial hypercholesterolemia
In familial hypercholesterolemia, the total cholesterol level is high. People may have inherited one abnormal gene or they may have inherited two abnormal genes, one from each parent. People who have two abnormal genes (homozygotes) are more severely affected than people who have only one abnormal gene (heterozygotes). About 1 in 200 people are heterozygotes, and 1 in 250,000 to 1 in 1 million people are homozygotes.
Affected people may have fatty deposits (eruptive xanthomas) in the tendons at the heels, knees, elbows, and fingers. Rarely, xanthomas appear by age 10. Familial hypercholesterolemia can result in rapidly progressive atherosclerosis and early death due to coronary artery disease. Children with two abnormal genes may have a heart attack or angina by age 20, and men with one abnormal gene often develop coronary artery disease between ages 30 and 50. Women with one abnormal gene are also at increased risk, but the risk usually starts about 10 years later than in men. People who smoke or have high blood pressure, diabetes, or obesity may develop atherosclerosis at even younger ages.
Treatment of familial hypercholesterolemia begins with following a diet that is low in saturated fats and cholesterol. When applicable, losing weight, stopping smoking, and increasing physical activity are advised. One or more lipid-lowering drugs are usually needed. Some people require apheresis, a method of filtering the blood to lower LDL cholesterol levels. Some people with homozygous familial hypercholesterolemia may benefit from liver transplantation. Early diagnosis and treatment can decrease the increased risk of heart attack and stroke.
Familial hypertriglyceridemia
In familial hypertriglyceridemia, triglyceride levels are high. This disorder affects about 1% of people. In some families affected by this disorder, atherosclerosis tends to develop at a young age, but in others, it does not.
Losing weight, if necessary, and limiting alcohol and carbohydrate consumption often lower triglyceride levels to normal. If these measures are ineffective, use of a lipid-lowering drug can help. For people who also have diabetes, good control of the diabetes is important.
Hypoalphalipoproteinemia
In hypoalphalipoproteinemia, the HDL cholesterol level is low. Many different genetic abnormalities can cause the low HDL level. Since medications that raise HDL cholesterol do not decrease the risk of atherosclerosis, hypoalphalipoproteinemia is treated by lowering LDL cholesterol.
Lipoprotein lipase deficiency and apolipoprotein CII deficiency
Lipoprotein lipase deficiency and apolipoprotein CII deficiency are rare disorders caused by the lack of certain proteins needed for the removal of triglyceride-containing particles. In these disorders, the body cannot remove chylomicrons from the bloodstream, resulting in very high triglyceride levels. Without treatment, levels are often considerably higher than 1,000 mg/dL (11 mmol/L) and can cause pancreatitis.
Symptoms appear during childhood and young adulthood. They include
Recurring bouts of abdominal pain
Enlargement of the liver and spleen
Pinkish yellow bumps in the skin on the elbows, knees, buttocks, back, front of the legs, and back of the arms
These bumps, called eruptive xanthomas, are deposits of fat. Eating fats worsens symptoms. Although this disorder does not lead to atherosclerosis, it can cause pancreatitis, which is occasionally fatal.
People who have these disorders must strictly limit the amount of all types of fat—saturated, unsaturated, and polyunsaturated—in their diet. People may need to take vitamin supplements to make up for nutrients missing from their diets. There are some therapies in development for treatment of lipoprotein lipase deficiency and apolipoprotein CII deficiency.
Secondary dyslipidemia
Secondary causes contribute to many cases of dyslipidemia.
The most important secondary cause of dyslipidemia is
A sedentary lifestyle with excessive dietary intake of total calories, saturated fat, cholesterol, and trans fats (see sidebar Types of Fat)
Some other common secondary causes include the following:
Having diabetes mellitus
Consuming large amounts of alcohol
Having chronic kidney disease
Having hypothyroidism
Having primary biliary cirrhosis
Using certain medications
Some people are more sensitive to the effects of diet than others, but most people are affected to some degree. One person can eat large amounts of animal fat, and the total cholesterol level does not rise above desirable levels. Another person can follow a strict low-fat diet, and the total cholesterol does not fall below a high level. This difference seems to be mostly genetically determined. A person’s genetic makeup influences the rate at which the body makes, uses, and disposes of these fats. Also, body type does not always predict levels of cholesterol. Some overweight people have low cholesterol levels, and some thin people have high levels. Eating excess calories can result in high triglyceride levels, as can consuming large amounts of alcohol.
Did You Know...
|
Some disorders cause lipid levels to increase. Diabetes that is poorly controlled or chronic kidney disease can cause total cholesterol levels or triglyceride levels to increase. Some liver disorders (particularly primary biliary cirrhosis) and an underactive thyroid gland (hypothyroidism) can cause the total cholesterol level to increase.
Use of medications such as estrogenshuman immunodeficiency virus (HIV) infection and AIDS can cause cholesterol and/or triglyceride levels to increase.
Cigarette smoking, HIV infection, poorly controlled diabetes, or kidney disorders (such as nephrotic syndrome) may contribute to a low HDL cholesterol level. Medications such as beta-blockers and anabolic steroids can lower the HDL cholesterol level.
Symptoms of Dyslipidemia
High lipid levels in the blood usually cause no symptoms. Occasionally, when levels are particularly high, fat is deposited in the skin and tendons and forms bumps called eruptive xanthomas. Sometimes people develop opaque white or gray rings at the edge of the cornea. Very high triglyceride levels can cause the liver or spleen to enlarge, a tingling or burning sensation in the hands and feet, difficulty breathing, and confusion and may increase the risk of developing pancreatitis. Pancreatitis can cause severe abdominal pain and is occasionally fatal.

Image courtesy of Michael H. Davidson, MD.

Image courtesy of Michael H. Davidson, MD.

© Springer Science+Business Media

Image courtesy of Michael H. Davidson, MD.

© Springer Science+Business Media


Image courtesy of Michael H. Davidson, MD.

Image courtesy of Michael H. Davidson, MD.


© Springer Science+Business Media


Image courtesy of Michael H. Davidson, MD.


© Springer Science+Business Media
Diagnosis of Dyslipidemia
Blood tests to measure cholesterol levels
Levels of total cholesterol, LDL cholesterol, HDL cholesterol, and triglycerides—the lipid profile—are measured in a blood sample. Because consuming food or beverages may cause triglyceride levels to increase temporarily, people must fast at least 12 hours before the blood sample is taken.
When lipid levels in the blood are very high, special blood tests are done to identify the specific underlying disorder. Specific disorders include several hereditary disorders (primary dyslipidemias), which produce different lipid abnormalities and have different risks.
Did You Know...
|
Screening for Dyslipidemia
The fasting lipid profile, is the levels of total cholesterol, triglycerides, LDL cholesterol, and HDL cholesterol measured after a person fasts for 12 hours. Doctors usually do this test every 5 years starting at age 20 as part of assessing whether the person is at risk of coronary artery disease.
In addition to measuring lipid levels, doctors also screen for other risk factors for cardiovascular disease, such as high blood pressure, diabetes, or a family history of high lipid levels.
In children and adolescents, screening with a fasting lipid profile is recommended between the ages of 2 and 8 years if the child has risk factors, such as a family member with severe dyslipidemia or one who developed coronary artery disease at a young age. In children with no risk factors, screening with a non-fasting lipid profile is usually done once before the child reaches puberty (usually between age 9 to 11) and once more between the ages of 17 to 21.
Treatment of Dyslipidemia
Lose weight
Exercise
Decrease saturated fats in the diet
Often lipid-lowering drugs
Usually, the best treatment for people is to lose weight if they are overweight, stop smoking if they smoke, decrease the total amount of saturated fat and cholesterol in their diet, increase physical activity, and then, if necessary, take a lipid-lowering drug.
Regular physical activity can help lower triglyceride levels and increase the HDL cholesterol level. An example is walking briskly for at least 30 minutes daily.
Treating children may be challenging. The American Academy of Pediatrics and the National Heart, Lung, and Blood Institute recommend treatment for some children with high lipid levels. Diet changes are recommended. Lipid-lowering drugs may be given to some children with very high lipid levels who do not respond to changes in diet, particularly children with familial hypercholesterolemia.
Lipid-lowering diet
A diet low in saturated fat and cholesterol can lower the LDL cholesterol level. However, people with high triglyceride levels also need to avoid consuming large amounts of sugar (whether in foods or beverages), refined flour (such as is used in most commercial baked goods), and starchy foods (such as potatoes and rice).
The type of fat consumed is important (see Types of Fat). Fats may be saturated, polyunsaturated, or monounsaturated. Saturated fats increase cholesterol levels more than other forms of fat. Saturated fats should provide no more than 5 to 7% of total calories consumed each day. Polyunsaturated fats (which include omega-3 fats and omega-6 fats) may help decrease levels of triglycerides and LDL cholesterol in the blood. The fat content of most foods is included on the label of the container.
Large amounts of saturated fats occur in meats, egg yolks, full-fat dairy products, some nuts (such as macadamia nuts), and coconut. Vegetable oils contain smaller amounts of saturated fat, but only some vegetable oils are truly low in saturated fats.
Margarine, which is produced from polyunsaturated vegetable oils, is usually a healthier substitute for butter, which is high in saturated fat (about 60%). However, stick margarines (and some processed foods) contain trans fats, which may increase LDL (bad) cholesterol levels and lower HDL (good) cholesterol levels. Margarines made primarily from liquid oil (squeeze or tub margarines) contain less saturated fat than butter, contain no cholesterol, and contain fewer trans fats than stick margarines. Margarines (and other food products) that contain plant stanols or sterols can help lower total and LDL cholesterol levels.
Did You Know...
|
Lipid-lowering drugs
Treatment with lipid-lowering drugs depends not only on the lipid levels but also on whether coronary artery disease, diabetes, or other major risk factors for coronary artery disease are present. For people who have coronary artery disease or diabetes, the risk of heart attack or stroke can be decreased by the use of the lipid-lowering drugs called statins. People who have very high cholesterol levels or who have other high risk factors for heart attack or stroke also may benefit from taking lipid-lowering drugs.
There are different types of lipid-lowering drugs:
Statins
Cholesterol absorption inhibitors
Bile acid binders
PCSK9 (proprotein convertase subtilisin/kexin type 9) inhibitors
Fibric acid derivatives
Supplements of omega-3 fats
Each type lowers lipid levels by a different mechanism. Consequently, the different types of drugs have different side effects and may affect lipid levels differently. Following a diet low in saturated fat when drugs are used is recommended.
Lipid-lowering drugs do more than lower lipid levels—they can also prevent coronary artery disease. In addition, statins have been shown to reduce the risk of early death.
People with very high triglyceride levels and who are at risk of pancreatitis may need both diet changes and triglyceride-lowering drugs, usually a fibrate or prescription omega-3 fatty acids.
Procedures to reduce cholesterol
Medical procedures that lower cholesterol levels are reserved for people with very high levels of LDL cholesterol that do not respond to diet and lipid-lowering drugs. Such people include those with familial hypercholesterolemia. LDL apheresis is the most commonly done procedure. LDL apheresis is a non-surgical procedure where blood is drawn from the person and the LDL component is separated from the rest of the blood in a special machine. The blood (minus the LDL component) is then returned to the person.
Treating causes of elevated cholesterol
Any conditions that cause or are risk factors for elevations in cholesterol levels also need to be treated. So people with diabetes should carefully control their blood glucose levels. Kidney disease, liver disease, and hypothyroidism are also treated. If a drug is causing the cholesterol elevation, doctors may give the person a lower dose or a different drug instead.
Monitoring treatment
Doctors usually do blood tests 2 to 3 months after treatment has started to determine whether lipid levels are decreasing. Once lipid levels have decreased sufficiently, doctors do blood tests once or twice a year. Doctors no longer use specific targets for lipid levels. Instead, doctors try to lower the lipid levels by a certain percentage, typically about 30 to 50%.
Because some lipid-lowering drugs can sometimes cause muscle and liver problems, doctors usually do blood tests when the person starts drug therapy. Then, if the person develops side effects, initial (baseline) measurements are available for comparison.
More Information
Healthy Children: Cholesterol Levels in Children and Adolescents: A parenting site sponsored by the American Academy of Pediatrics provides information on healthy cholesterol levels for children and adolescents, screening information, and diet tips
National Heart Lung and Blood Institute: Blood Cholesterol: Provides information on ways to maintain healthy blood cholesterol levels






