Acute otitis media is a bacterial or viral infection of the middle ear.
Acute otitis media often occurs in people with a cold or allergies.
The infected ear is painful.
Doctors examine the eardrum to make the diagnosis.
Certain routine childhood vaccinations can reduce the risk of acute otitis media.
The infection is sometimes treated with antibiotics.
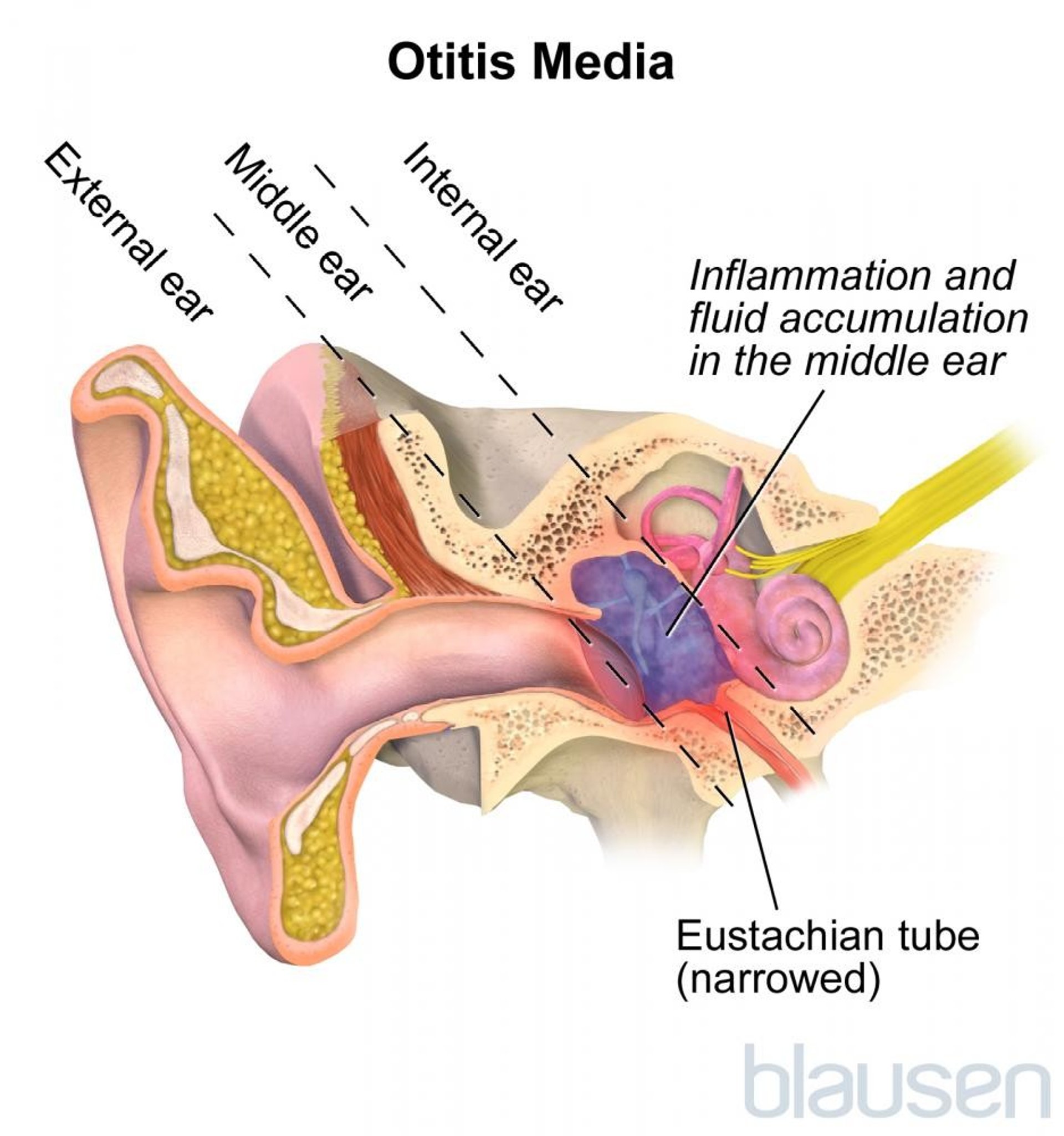
Acute otitis media results from infection by viruses or bacteria, often as a complication of the common cold or of allergies. Although acute otitis media can occur at any age, it is most common between the ages of 3 months and 3 years. Acute otitis media often occurs during this age range because structures in the middle ear (such as the eustachian tube) are immature and function less efficiently than in adults. Symptoms and treatment are similar in adults and older children (for acute otitis media in younger children, see Acute Middle Ear Infection in Children).

Conditions that increase the risk of otitis media (risk factors) include
Living in a household where people smoke
Having many relatives who have had otitis media
Living in an area with heavy air pollution
Being bottle fed, rather than breastfed
Being in a day care center
Rarely, bacterial otitis media spreads to nearby structures such as the mastoid bone behind the ear (mastoiditis) or the inner ear. Spread into the brain is extremely rare, but some people develop meningitis or a collection of pus (abscess) in or around the brain.

Symptoms of Acute Otitis Media
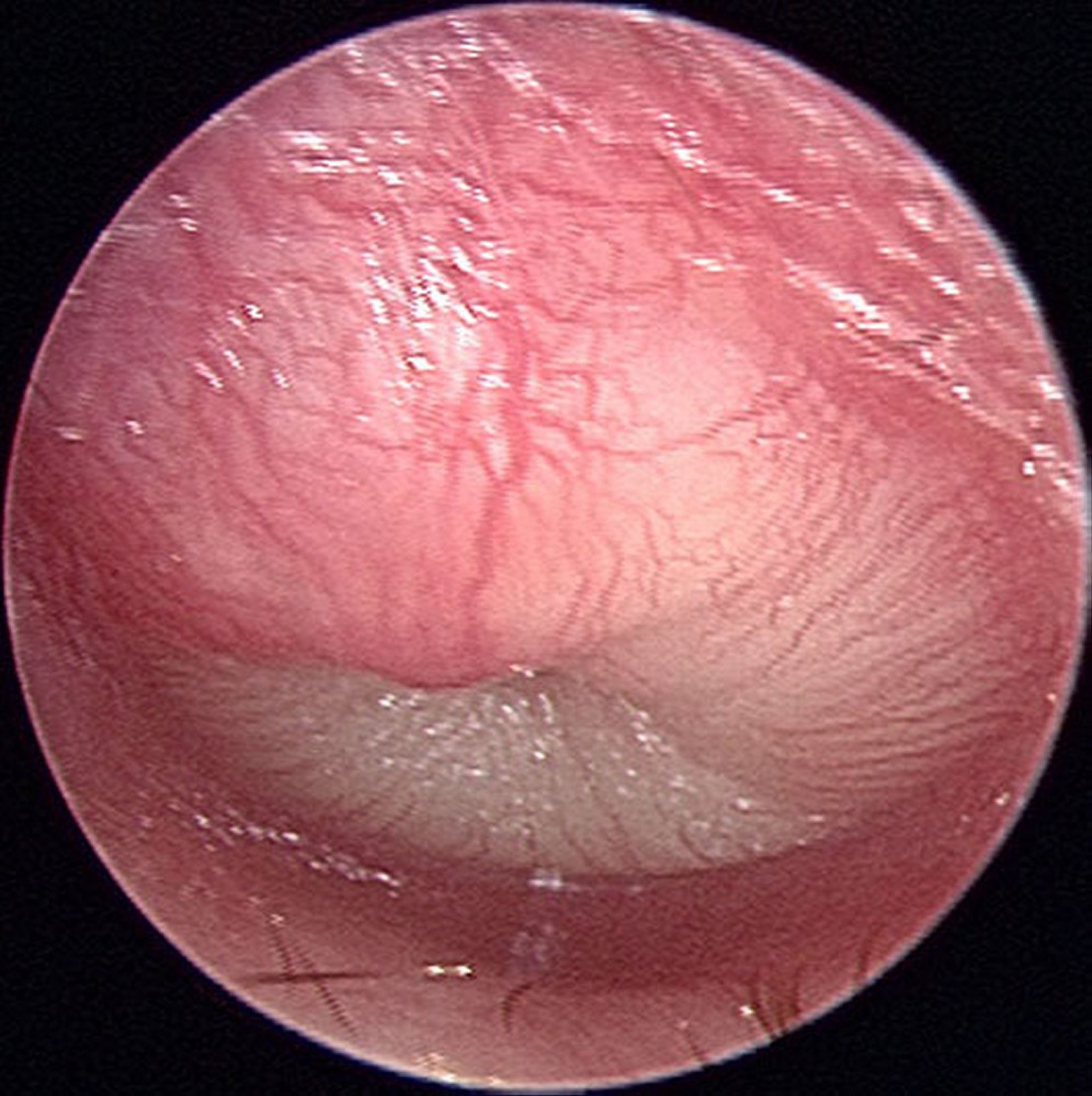
In people with acute otitis media, the infected ear is painful (see Earache), with a red, bulging eardrum. Many people have hearing loss. Infants may simply be cranky or have difficulty sleeping. Fever, nausea, vomiting, and diarrhea often occur in young children. The bulging eardrum sometimes ruptures, causing pus to drain from the ear, sometimes with relief of ear pain.

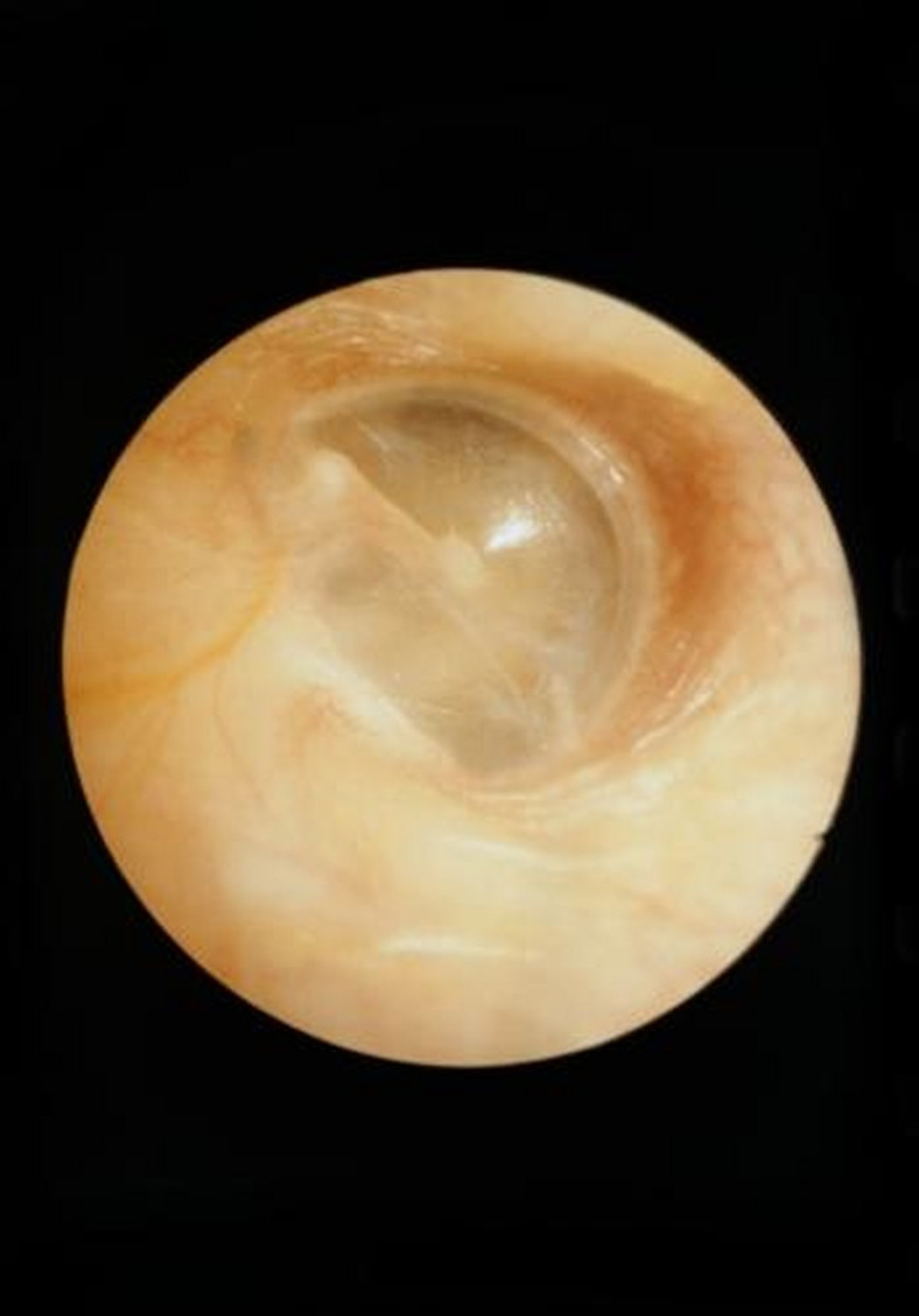
CLINICA CLAROS/SCIENCE PHOTO LIBRARY

© Springer Science+Business Media
If the infection spreads, people may have a severe headache, confusion, or impaired brain function.
Diagnosis of Acute Otitis Media
A doctor's evaluation
Doctors use an otoscope (a handheld light) to examine the ear canal and eardrum. If otitis media is present, pus may be visible in the middle ear behind the eardrum.
Treatment of Acute Otitis Media
Pain relievers
Antibiotics if needed
Children are young (for example, younger than 6 months).
Symptoms are severe.
Symptoms do not lessen after 72 hours.
Otitis media recurs frequently.
Some experts say that children age 6 to 23 months with acute otitis media that is in only one ear and is not severe and older children can start treatment with or without antibiotics. If antibiotics are not used initially, they are given if the child is worse or does not feel better after 48 to 72 hours have passed since symptoms began.
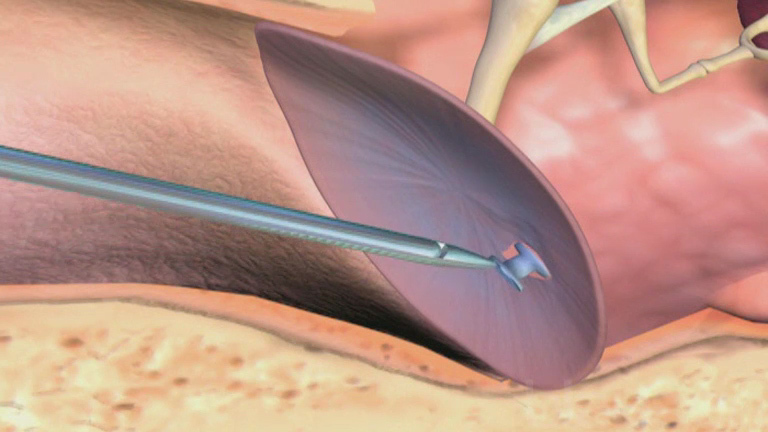
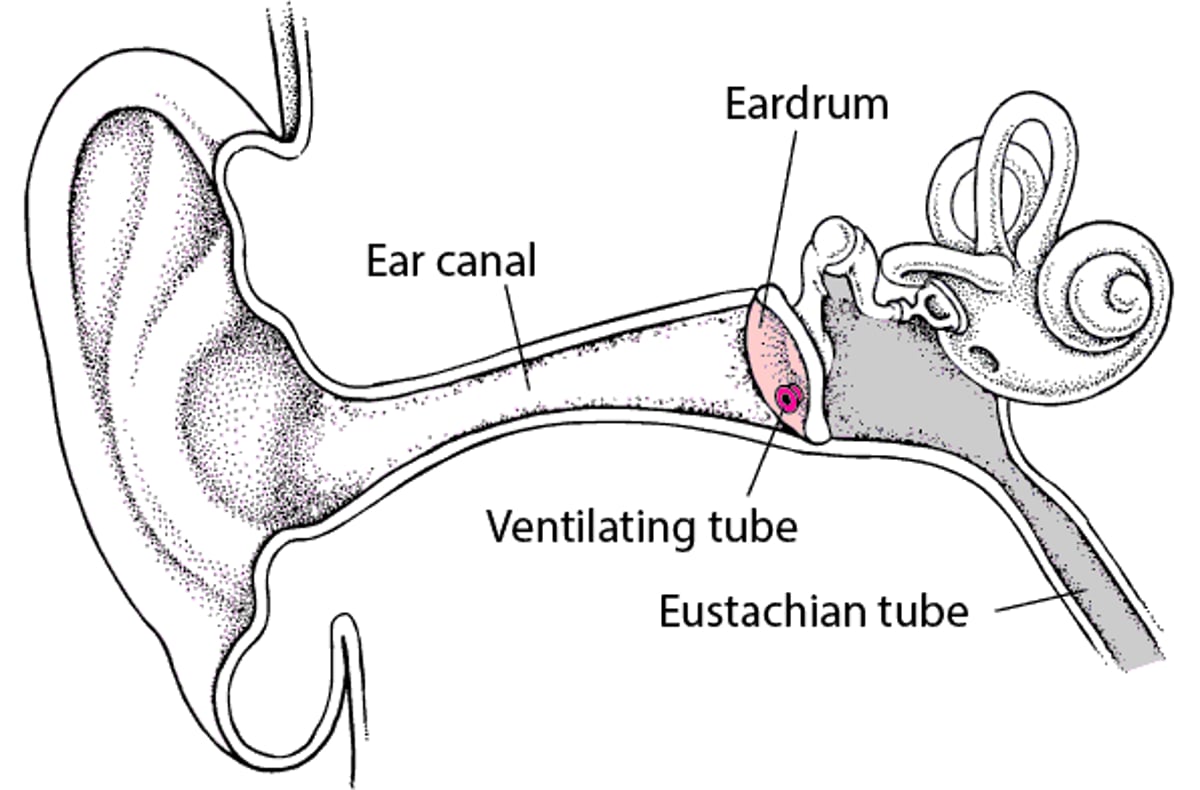
If a person has severe or persistent pain and fever and the eardrum is bulging, myringotomy may be done. For this procedure, an opening is made through the eardrum to allow fluid to drain from the middle ear. The opening, which does not affect hearing, usually heals without treatment. People who have repeated bouts of otitis media may need to have drainage tubes (tympanostomy tubes) placed in their eardrums (see figure Myringotomy).
Myringotomy: Treating Recurring Ear Infections
During a myringotomy, doctors make a small opening in the eardrum to allow fluid to drain from the middle ear. Then they place a tiny, hollow plastic or metal tube (tympanostomy tube, or ventilating tube) in the eardrum through the opening. These tubes balance the pressure in the environment with that in the middle ear. Doctors recommend ventilating tubes for some children who have had recurring ear infections (acute otitis media) or recurring or persistent collections of fluid in their middle ears (chronic serous otitis media). Placement of ventilating tubes is a common surgical procedure that is done in a hospital or doctor’s office. General anesthesia or sedation is usually required. After the procedure, children usually go home within a few hours. Antibiotic ear drops are sometimes given after the procedure for about a week. The tubes usually come out on their own after about 6 to 12 months, but some types stay in longer. Tubes that do not come out on their own are removed by the doctor, sometimes under general anesthesia or sedation. If the opening does not close on its own, it may need to be closed surgically. Children with ventilating tubes may wash their hair and go swimming, but some doctors recommend children do not submerge their head in deep water without using earplugs. Drainage of fluid from the ears indicates an infection, and the doctor should be notified. |

Prevention of Acute Otitis Media
The risk of acute otitis media can be reduced by routine childhood vaccinations against pneumococci (with pneumococcal conjugate vaccine), Haemophilus influenzae type B (HiB), and influenza (flu). Infants should not sleep with a bottle because a bottle makes it easy for liquid to run through the eustachian tube into the middle ear. Secondhand smoke may increase the risk, so people should not smoke, especially in the house or around children.
Recurrent acute otitis media may be prevented by the insertion of drainage tubes (tympanostomy tubes).