Here for Good: The human element inspiring our cancer research
Learn how one doctor turned his family connection to cancer into a career driven by scientific innovation
May 27, 2022
Share this article
Advances in oncology research require a firm commitment to scientific investigation. Behind every innovation, there are countless researchers, doctors and clinicians who dedicate their lives to helping patients through scientific breakthroughs.
At Merck, Dr. Gregory Lubiniecki, vice president, oncology clinical research, is a senior leader who oversees cancer research. He’s also a practicing clinician, continuing to see patients — adding a human connection to his research.
For Lubiniecki, having a “one-on-one connection” with patients is important both personally and professionally, and helps to keep the patient experience at the forefront when designing clinical studies.
Dr. Lubiniecki’s drive to pursue a career in oncology was motivated by his family’s experience with cancer — watching his mother go through surgery and chemotherapy while he was in high school — and his own scientific curiosity. “The complexity of the molecular biology involved in cancer was very intriguing to me,” he said.
Dr. Lubiniecki and his team play a critical role in advancing Merck’s effort to help save and improve lives around the world through leading-edge science. With an ongoing connection to patients and his research firmly focused on the future, Dr. Lubiniecki is excited about where cancer care may go next.
“I’m very excited about several clinical projects that are going to try and improve the lives of patients who are fighting cancer.”
Dr. Gregory Lubiniecki
Watch the video to learn more about Dr. Lubiniecki
The Mectizan Donation Program is the longest-running, disease-specific drug donation program of its kind
May 25, 2022
Share this article
Our commitment: “as much as needed, for as long as needed…"
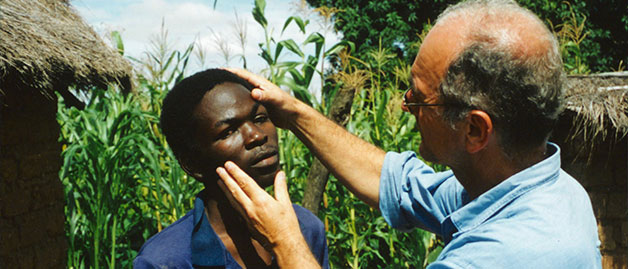
For centuries, river blindness — also known as onchocerciasis — plagued remote communities in Africa, Latin America and Yemen, and there was no answer to this affliction.
This all began to change in the mid-to-late 1970s when Dr. William Campbell of Merck Research Laboratories suggested the use of ivermectin (later named Mectizan) for river blindness in humans. Following the breakthrough lab work by Dr. Campbell, another Merck researcher, Dr. Mohammed Aziz, championed the clinical development of Mectizan. Dr. Aziz led the collaboration with the World Health Organization (WHO) in the early 1980s to design and implement field studies in West Africa that, ultimately, proved the effectiveness of the drug against river blindness.
In 1987, Merck committed to donate Mectizan – as much as needed, for as long as needed – with the goal to help eliminate river blindness.
MDP partners include: World Health Organization, the Task Force for Global Health, ministries of health, non-governmental development organizations, academic institutions and local communities in endemic communities.
A ground-breaking public-private partnership
In order to reach this goal, Merck leaders recognized that many organizations with unique skills would need to work together as a team. To enable this collaboration, Merck established the Mectizan Donation Program (MDP), a ground-breaking public-private partnership. Operating from the Atlanta-based Task Force for Global Health, the MDP coordinates technical and operational activities between Merck, WHO, endemic countries, and a range of public and private stakeholders.
Building on the successful implementation of the river blindness program, in 1998 Merck expanded its commitment to include donating Mectizan for another neglected tropical disease, lymphatic filariasis, also known as elephantiasis, in African countries and Yemen where it co-exists with river blindness. For lymphatic filariasis, Mectizan is administered with albendazole, a drug donated by GSK.
In November 2017, in support of new WHO guidelines, Merck announced an expansion of the program to reach up to an additional 100 million people per year through 2025 as part of the global effort to eliminate lymphatic filariasis.
More than thirty years later, the results of the MDP speak for themselves. Several countries in Africa are making significant progress towards eliminating both diseases. In Latin America, four countries – Colombia, Ecuador, Mexico and Guatemala – have received WHO verification of river blindness elimination. Lymphatic filariasis has now been eliminated in Togo, Yemen and Malawi. Both river blindness and lymphatic filariasis are on WHO’s list of neglected tropical diseases targeted for elimination globally.
Pioneering a community-directed approach
Today, the MDP is the longest-running, disease-specific drug donation program of its kind and has been influential in the development of a number of other drug donation programs. And, the MDP’s community-directed strategy used to distribute Mectizan has enabled add-on health services to be introduced in remote communities where health services are limited. The program reaches more than 300 million people in the affected areas annually, with more than 4.4 billion treatments donated since 1987.
People in the communities are an integral part of the distribution process in 49 countries where Mectizan has been distributed.
According to Uche Amazigo, former director of the African Programme for Onchocerciasis Control, “by engaging the people, the treatment coverage increased significantly.”
“This pioneering program has changed the face of global health over the past three decades,” said Yao Sodahlon, head of the MDP. “When I visit communities where Mectizan is donated, I can see how the program has helped alleviate suffering and allowed people to live better and healthier lives.”
What are river blindness and lymphatic filariasis?
River blindness (onchocerciasis)
River blindness is one of the leading causes of preventable blindness worldwide. Transmitted through the bite of black flies — which live and breed near fast-flowing streams and rivers — and can cause intense itching, permanent skin and eye lesions and, over time, blindness. It has historically been prevalent in remote rural areas of 36 countries (in Africa, Latin America, and in Yemen.)
Lymphatic filariasis (LF)
Also known as elephantiasis, LF results in disfiguring swelling in the limbs and genitals. Parasitic infection spread by mosquitoes and damages the human lymphatic system. More than 1.3 billion people are at risk, and 30 percent of those infected live in Africa.
35 years later, results of this program speak for themselves
More than 4.4 billion cumulative treatments
Donations to 49 countries
Through the efforts of a variety of partners, more than 4.4 billion treatments have been donated to 49 countries in Africa, Latin America, Eastern Mediterranean, Asia, and South Pacific. River blindness transmission has been interrupted – meaning no new cases have been identified – in four of the six affected countries in Latin America and regions in five African countries. The program reaches more than 300 million people annually.
Today, the MDP is the longest-running, disease-specific drug donation program of its kind.
“We are proud of the positive difference that the Mectizan Donation Program has made in the lives of so many people, their families and communities, and health care systems over the years. Together, with our alliance of partners, we will continue to support endemic countries in their commitment to eliminate these devastating diseases.”
Rob Davis, CEO and President, Merck
Explore our history of helping bring treatment to those afflicted by river blindness and elephantiasis
1978
Dr. William Campbell of Merck Research Laboratories suggests the use of Mectizan (ivermectin) against onchocerciasis (river blindness) in humans.
1981
The first human clinical trials begin in Dakar with the first patient receiving a single dose.
1987
Merck CEO Dr. Roy Vagelos announces the company’s commitment to donate Mectizan to treat river blindness — as much as needed, for as long as needed — the MDP is formed.
1988
The Mectizan Expert Committee meets for the first time to establish the strategy for distribution and the donation review process. Mectizan has been produced at the MSD plant in Haarlem, the Netherlands, since the beginning of the program.
1991
Merck, the MDP Secretariat and WHO establish the Non-Governmental Development Organization (NGDO) Coordination Group for Onchocerciasis Control. NGDOs play a critical role in Mectizan distribution through their work with ministries of health and local communities, expertise in program management, and financial support.
1993
The Onchocerciasis Elimination Program for the Americas (OEPA), formed by the River Blindness Foundation and currently sponsored by The Carter Center, brings together the ministries of health of six countries in Latin America affected by onchocerciasis.
1995
WHO, the World Bank, international NGOs, and 19 African countries partner to create the African Program for Onchocerciasis Control (APOC), providing a structure for financial support and coordination of river blindness control efforts.
1998
Merck begins a partnership with GSK to expand the MDP to include the elimination of LF, commonly referred to as elephantiasis, in African countries and in Yemen.
Merck and the MDP celebrate the 100 millionth treatment in Uganda.
1999
The iconic river blindness statue, “Sightless Among Miracles” by sculptor R. T. Wallen, is dedicated at WHO headquarters in Switzerland. Identical statues are also found at The Carter Center (Georgia, USA), the World Bank (Washington, D.C., USA), the Royal Tropical Institute (Amsterdam, the Netherlands), Merck (New Jersey, USA) and Lions Club International Foundation (Illinois, USA).
2002
In Tanzania, Merck CEO Raymond
Gilmartin celebrates the 250 millionth
treatment distributed.
2008
The Pan American Health Organization passes a resolution calling for the interruption of transmission of river blindness in the Americas by the year 2012.
WHO confirms the potential for elimination of river blindness in some parts of Africa through current treatment strategies.
2010
Merck reaffirms its commitment to the MDP. Merck “will continue to [donate Mectizan] until river blindness becomes a disease of the past,” said Merck CEO Richard T. Clark.
2011
Colombia becomes the first country to apply for WHO certification for the elimination of onchocerciasis transmission after suspending treatment with Mectizan in 2007.
2012
Merck CEO Kenneth C. Frazier commemorates the 25th anniversary of the MDP at a celebratory event in London.
2013
WHO verifies that Colombia has eliminated onchocerciasis, thus becoming the first country in the world to achieve this goal.
2014
WHO verifies the elimination of onchocerciasis in Ecuador. Ecuador worked in partnership with the MDP and a number of other organizations and now becomes the second country in the world to be free of this disease.
2015
WHO verifies the elimination of onchocerciasis in Mexico, the third country in the world to be free of river blindness.
Dr. William C. Campbell, Ph.D., is jointly awarded the Nobel Prize in Physiology or Medicine for the discovery of avermectin, which led to a treatment for river blindness. Dr. Campbell performed his Nobel Prize-winning work at Merck Research Laboratories in Rahway, N.J., where he worked from 1957 until his retirement in 1990.
2016
WHO verifies the elimination of onchocerciasis in Guatemala thanks to a partnership with the MDP and a number of other organizations. With this milestone, four of the six countries in the Americas historically at-risk for river blindness now have verified elimination of the disease.
2017
Togo becomes the first country in Africa recognized by WHO to have eliminated LF as a public health problem.
Merck announces an expansion of the MDP to reach up to an additional 100 million people per year through 2025 as part of the global effort to eliminate LF.
2019
WHO verifies the elimination of LF as a public health problem in Yemen. The Mectizan Expert Committee meets in Togo and presents the Ministry of Health with the Lymphatic Filariasis Elimination Award.
2020
WHO verifies the elimination of LF as a public health problem in Malawi.
2021
MDP and Merck announce a $500,000 donation to strengthen laboratory capacity to support onchocerciasis elimination in Africa in partnership with WHO’s Collaborating Centre for Onchocerciasis Diagnostics at the College of Public Health, University of South Florida.
2022
Merck and MDP mark the 35th anniversary of the program.
How Wilson, N.C., plays a critical role in our commitment to supply
Meet the North Carolina-based manufacturing team that’s producing and packaging our investigational oral antiviral COVID-19 medicine
March 2, 2022
Share this article
From the earliest stages of the COVID-19 pandemic, we knew we had a responsibility to rise to the challenge of this unique moment. That’s why our teams mobilized like never before to ensure we were ready to address a global need.
In late 2020, our manufacturing teams began utilizing our global supply network — including sites in nine countries across three continents — to start production of our investigational oral antiviral COVID-19 medicine. This monumental effort made it possible for us to produce 10 million courses of therapy in 2021, with at least another 20 million on track for 2022.
A major part of that effort takes place in Wilson, North Carolina, where our colleagues are working tirelessly to carry out our mission and ensure supply during this crucial time.
“This is a perfect example of the company coming together as one team with a single goal,” said Francisco Toste, associate vice president, plant management at the Wilson site. “I am proud to work for our great company because of the impact that we make for patients around the world in helping them combat serious disease.”
Meet the team in Wilson behind this heroic effort:
When the world needs us, together we rise to the challenge
Merck CEO & President Rob Davis shares news with colleagues about our investigational COVID-19 medicine
December 23, 2021
Share this article
Dear Colleagues,
Today, we announced the emergency use authorization of molnupiravir, our investigational oral antiviral COVID-19 medicine, by the U.S. Food and Drug Administration (FDA). The action today taken by the FDA to authorize a pill for COVID-19 treatment that can be taken at home marks an important milestone in the pandemic. With this news, certain patients in the U.S. in consultation with their health care providers will soon be able to access this medicine, consistent with its authorized use.
As I reflect on the significance of this moment and the efforts that we have undertaken, united as one team, I am extremely proud of the innovation, hard work and commitment that we’ve demonstrated to bring this important medicine forward. Since the beginning, we committed to help fight the pandemic and protect global health by ensuring that any medicine or vaccine we developed for COVID-19 would be broadly available, and we have acted with urgency and diligence to do just that.
This is certainly a moment for reflection and recognition of the many milestones we achieved throughout this journey as a team, in partnership with Ridgeback, clinical trial investigators and participants, and others. We completed a successful clinical trial for an oral antiviral COVID-19 medicine; we scaled up manufacturing to produce more courses, sooner, than we had ever done before; and, we entered voluntary licensing agreements with generic manufacturers and the Medicines Patent Pool to create rapid and equitable global access for this medicine in low- and middle-income countries.
It is amazing and rewarding to see what we can accomplish – together – with focus, agility and with patients at the center of our efforts. I want to thank our collaborators, and each and every one of you, for relentlessly working to bring yet another impactful medicine forward in service of our mission to save and improve lives.
This medicine has not been approved in the U.S., but has been authorized for emergency use by the U.S. Food and Drug Administration (FDA) under an Emergency Use Authorization (EUA). The authorized use of the product is described in the EUA and authorized labeling. The emergency use of this product is only authorized for the duration of the declaration that circumstances exist justifying the authorization of the emergency use of drugs and biological products during the COVID-19 pandemic under Section 564(b)(1) of the Federal Food, Drug, and Cosmetic Act, 21 U.S.C. § 360bbb-3(b)(1), unless the declaration is terminated or authorization revoked sooner.
Mitos y realidades sobre la enfermedad neumocócica
Analizamos posibles percepciones erróneas sobre la enfermedad neumocócica y su impacto en niños y adultos.
September 9, 2021
Share this article
Enfermedad neumocócica se llama a cualquier infección causada por una bacteria llamada Streptococcus pneumoniae, también conocida como neumococo. Las infecciones neumocócicas pueden incluir infecciones del oído y la nariz, neumonía e infecciones del torrente sanguíneo (bacteriemia).
Mito: La enfermedad neumocócica no es grave.
Realidad: La infección neumocócica contribuye a la muerte y a la enfermedad en todo el mundo.
La neumonía neumocócica, por ejemplo, es una de las principales causas infecciosas de muerte en niños pequeños alrededor del mundo. Como otro ejemplo, cada año en los EE. UU., la neumonía neumocócica causa un estimado de 150.000 hospitalizaciones.
Mito: La enfermedad neumocócica siempre es neumonía.
Realidad: La neumonía neumocócica (cuando se limita a los pulmones) y la neumonía bacteriémica (neumonía con bacteriemia) son solo dos tipos de enfermedades causadas por bacterias neumocócicas.
Además de las enfermedades más comunes, como la sinusitis e infecciones del oído medio, los casos más graves de enfermedad neumocócica ocurren cuando la bacteria neumocócica invade partes del cuerpo que normalmente no tienen gérmenes, como el torrente sanguíneo en el caso de la bacteriemia. Esto se llama enfermedad neumocócica “invasiva”.
Además, la meningitis neumocócica es una infección rara pero grave de la membrana que cubre el cerebro y la médula espinal. Esto puede provocar complicaciones a largo plazo, como daño cerebral, pérdida de la audición y convulsiones.
Mito: Hay solo una cepa de bacteria que causa la enfermedad neumocócica.
Realidad: Existen numerosos tipo únicos de bacterias neumocócicas, denominados serotipos.
Los tipos de bacteria se diferencian dediversasmaneras: algunos son más prevalentes en un país que en otro, otros es más probable que causen ciertos tipos de enfermedades neumocócicas, y otros es más probable que sean responsables de los casos más graves.
Mito: La enfermedad neumocócica afecta a todas las personas por igual.
Realidad: Cualquier persona puede contraer la enfermedad neumocócica, pero algunas personas corren más riesgo.
Si bien los adultos y los niños sanos pueden padecer de la enfermedad neumocócica, las personas con más riesgo incluyen niños de menos de 2 años de edad, adultos mayores de más de 65 años y personas con ciertas afecciones crónicas, como enfermedades del corazón, diabetes u enfermedad pulmonar obstructiva crónica (EPOC).
Mito: La COVID-19 y la neumonía neumocócica son lo mismo.
Realidad: La neumonía es una infección pulmonar que puede ser el resultado de una serie de causas, incluidos virus, bacterias y hongos.
Aunque la causa de la neumonía no siempre es la bacteria neumocócica, esta es una causa frecuente. A la neumonía neumocócica la causa una bacteria llamada Streptococcus pneumoniae, mientras que a la COVID-19 la causa un virus llamado SARS-CoV-2. Son distintas enfermedades, pero la neumonía neumocócica y la COVID-19 sí comparten ciertos factores de riesgo, incluidos la edad avanzada y ciertas afecciones médicas preexistentes.
Podcast: How to bridge diversity gaps in cancer clinical trials
Luther Clark talks with Lazarex Cancer Foundation's Dana Dornsife and Marya Shegog about increasing access among historically underrepresented communities
May 17, 2021
Share this article
Diversity in cancer clinical trials is essential to show if potential treatments are safe and work well for people of all different communities. That’s why it’s crucial to break down barriers and increase participation in cancer clinical trials among historically underrepresented communities.
In this podcast, Luther Clark, Merck’s deputy chief patient officer, speaks with the Lazarex Cancer Foundation’s founder and CEO, Dana Dornsife, and its health equity and diversity coordinator, Marya Shegog, about the work they’ve been doing — and the work that still needs to be done — to foster health equity through cancer clinical trials.
Forward-looking statement of Merck & Co., Inc., Rahway, N.J., USA
This website of Merck & Co., Inc., Rahway, N.J., USA (the “company”) includes “forward-looking statements” within the meaning of the safe harbor provisions of the U.S. Private Securities Litigation Reform Act of 1995. These statements are based upon the current beliefs and expectations of the company’s management and are subject to significant risks and uncertainties. There can be no guarantees with respect to pipeline candidates that the candidates will receive the necessary regulatory approvals or that they will prove to be commercially successful. If underlying assumptions prove inaccurate or risks or uncertainties materialize, actual results may differ materially from those set forth in the forward-looking statements.
Risks and uncertainties include but are not limited to, general industry conditions and competition; general economic factors, including interest rate and currency exchange rate fluctuations; the impact of pharmaceutical industry regulation and health care legislation in the United States and internationally; global trends toward health care cost containment; technological advances, new products and patents attained by competitors; challenges inherent in new product development, including obtaining regulatory approval; the company’s ability to accurately predict future market conditions; manufacturing difficulties or delays; financial instability of international economies and sovereign risk; dependence on the effectiveness of the company’s patents and other protections for innovative products; and the exposure to litigation, including patent litigation, and/or regulatory actions.
The company undertakes no obligation to publicly update any forward-looking statement, whether as a result of new information, future events or otherwise. Additional factors that could cause results to differ materially from those described in the forward-looking statements can be found in the company’s Annual Report on Form 10-K for the year ended December 31, 2024 and the company’s other filings with the Securities and Exchange Commission (SEC) available at the SEC’s Internet site (www.sec.gov).
No Duty to Update
The information contained in this website was current as of the date presented. The company assumes no duty to update the information to reflect subsequent developments. Consequently, the company will not update the information contained in the website and investors should not rely upon the information as current or accurate after the presentation date.